In vivo studies of titanium implant surface treatment by sandblasted, acid-etched and further anchored with ceramic of tetracalcium phosphate on osseointegration
Link: /uploads/arquivos/In-vivo-studies-of-titanium-implant-surface-treatment-by-sandblasted.pdf
Journal of the Australian Ceramic Society
https://doi.org/10.1007/s41779-018-00292-5
Jian-Chih Chen1,2 & Chia-Ling Ko3,4,5 & Dan-Jae Lin6,7 & Hui-Yu Wu3,4 & Chun-Cheng Hung4,8 & Wen-Cheng Chen3,4,6
Received: 15 August 2018 /Revised: 22 October 2018 /Accepted: 13 December 2018
# Australian Ceramic Society 2019
Abstract
The objective was to investigate and compare the osseointegrative responses of sandblasted/acid-etched (SLA) and calcium phosphate (CaP) implants in vivo. The CaP implant was prepared by control group of SLA surface modification and anchoring with sintering ceramic of tetracalcium phosphate (TTCP) to form a mechanical interlocking film. Customized screw Ti implants (size Ø 2.0 mm× 6 mm length) were utilized to histologically examine the bone-to-implant contact (BIC) after implantation. The implant stability quotient scales in the postoperative implants within femurs were recorded. Subsequently, the postoperative implants were scanned using microcomputed tomography (micro-CT), and the topography was examined microscopically to analyze the BIC conditions. The SLA and CaP implant groups showed increased bone mineral density (g/cm3) and BIC (%). Compared with the SLA implant, the CaP implant with TTCP improved the early osteointegration of the BIC at 1-month postoperation and demonstrated quantitative effects on the BIC at 1-month post-operation. SLA and CaP implants all showed good osseointegration through micro-CT analysis (1–6 months). The current findings suggest the CaP anchoring Ti surface demonstrated improvement in early stages of osseointegration and thus shows the potential clinical benefits of TTCP anchoring on Ti surfaces in bone-level solutions.
Conclusion
Both implants reached the healing and bone formation rates at osteoregeneration periods of 1, 2, 3, and 6 months. No gaps within their respective interfaces were grossly observed. However, comprehensive in vivo evaluation revealed that the osseointegration performance of the SLA with anchored CaP on the implant surface was better than that of the SLA only group in contact with the implant percentage at 1-month post-operation. The results of micro-CT measurements and histological analysis revealed improved healing trends and better bone-maintained level in the CaP implant group than in the SLA implant group at an earlier stage. New bone around the CaP implants can be regenerated and shorten the time required for osseointegration.
Our comments:
This is a SLA implant with no Calcium Phosphate, note the aluminum in white.
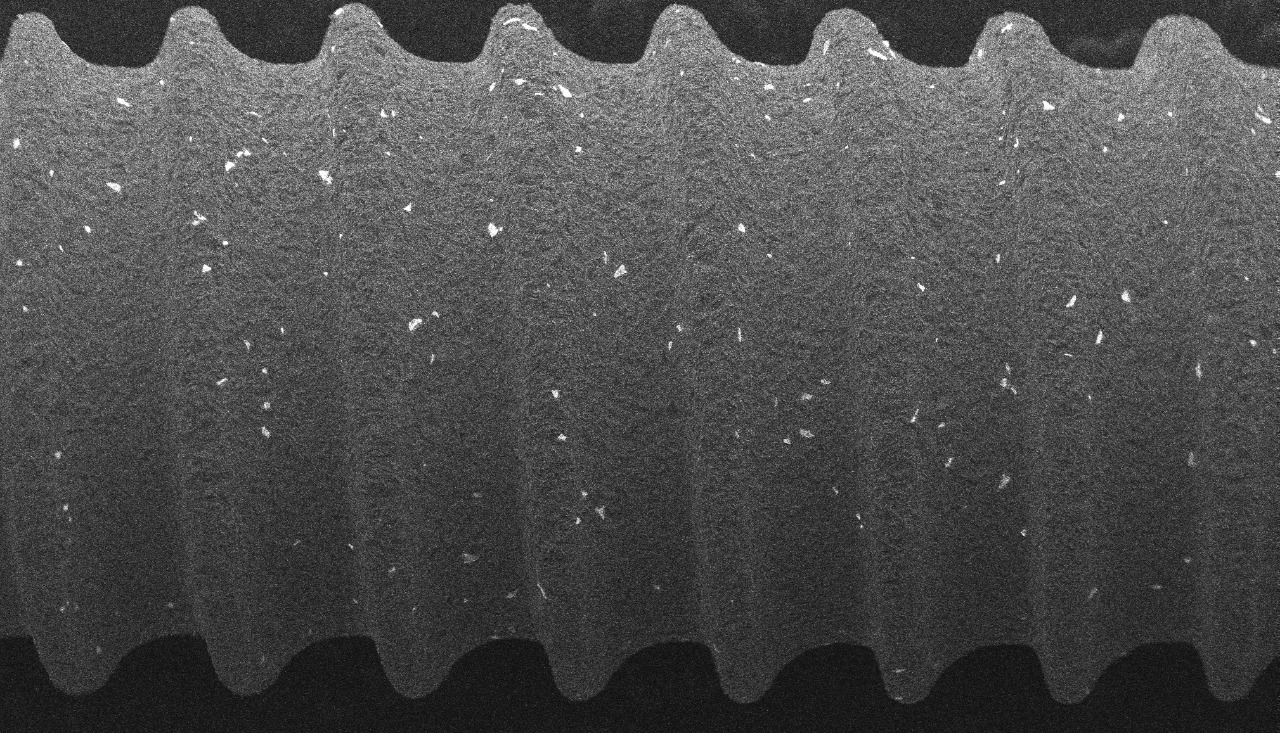
In this article, the researcher took 2 groups, one with pure unmodified SLA and one with modified SLA with CaP - calcium phosphate inclusion.
Obs: In this case, he used tetracalcium phosphate, it is different between hydroxyapatite and a mixture of calcium phosphate. HA has to have the crystal, if it do not have the crystal, it is just a phosphate and calcium mix.
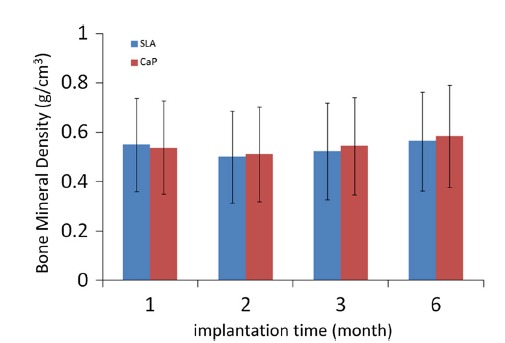
But anyway, see this chart of density?
In the first month the pure SLA showed higher, then the body was noticing the aluminum in the implant and as everyone already knows aluminium is linked to osteomalacia (soft bone), that is why from the second to the sixth month the SLA modified with the inclusion of the calcium and phosphate layer covering the parts with aluminum began to give higher density. Exactly why the bone don't like aluminum, but likes phosphorus and calcium.
Anyway, as much as it is just a layer of calcium phosphate, the implant with this layer is better because the body will first absorb this phosphate and calcium and then it will reach the aluminum. When it arrives in aluminum will lower the density and become an implant like SLA without modification.
But until then the implant that has CaP will have a longer survival.
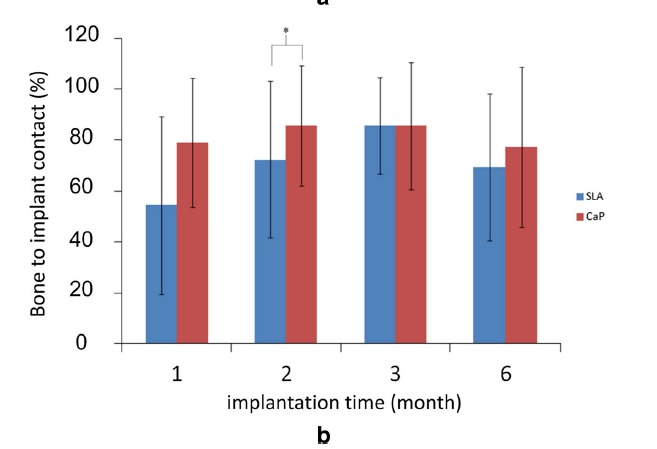
This is the BIC chart, notice that even though it has aluminum underneath, what is in contact with the bone is calcium phosphate on the surface. Bone likes phosphorus and calcium.
See the much higher BIC in the calcium phosphate SLA implant than in the aluminum contact implant.
Of course the aluminum is underneath but until the organism absorb the calcium phosphate to reach the aluminum the implant will last longer!